Spinal cord injury: effects on respiratory system
The spinal cord is the exclusive relay of sensory, motor and autonomic information between the CNS and the peripheries. The level of spinal cord injury determines whether individual organs will remain in communication with the brain.
Respiratory failure is common after spinal cord injury; respiratory complications are the most common cause of death.
With cervical and upper thoracic cord injury, the major cause of morbidity and mortality is alveolar hypoventilation combined with an inability to clear bronchial secretions.
Respiratory muscles are not affected with lumbar and low thoracic injuries, so
minimal respiratory impairment can be expected with these injuries.
The higher the spinal cord lesion, the greater the impact on ventilation:
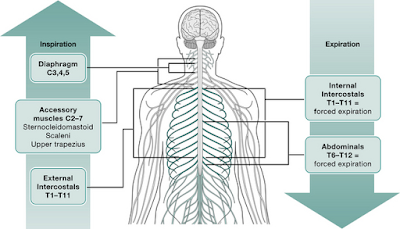
– Injury at C5 vertebral level and above
Paralysis of diaphragm and all respiratory muscles.
Gross ventilatory impairment requiring immediate ventilatory support.
Usually require long-term mechanical ventilation or phrenic nerve stimulation.
– Injury below C5 vertebral level
Does not directly affect diaphragmatic contraction (the phrenic nerve is formed by the C3, C4 and C5 nerve roots).
Diaphragmatic contraction is indirectly affected as intercostal muscle paralysis results in paradoxical movement of the chest wall – it is drawn inwards during diaphragmatic contraction.
Tidal volume may be unaffected due to intact diaphragmatic function but ability to cough and clear out of secretion is reduced due to decreased expiratory reserve volume as a result of denervation of intercostal and abdominal muscles.
Vital capacity reduces by up to 50%.
– Injury above T8 vertebral level
The loss of intercostal muscle tone reduces the outward spring of the chest wall.
The ‘bucket-handle’ movement is abolished and diaphragmatic contraction becomes the sole mechanism of inspiration.
The functional residual capacity, which reflects the volume at which the inward elastic recoil of the lung equals the outward spring of the chest wall, is therefore reduced.
Spinal cord injury alters lung mechanics in several ways that results in pulmonary complications:
Paralysis of the external intercostal muscles and the abdominal muscles:
- Results in markedly reduced forced expiratory gas flows and Forced expiratory volume in 1 sec.
- Reduction of Vital capacity, Expiratory reserve volume and Functional residual capacity.
- Cough is severely impaired, leading to impaired clearance of respiratory secretions.
Pulmonary oedema:
Neurogenic pulmonary edema may occur because of systemic and pulmonary vasoconstriction due to acute sympathetic overactivity, which subsequently causes acute translocation of blood into the pulmonary circulation and transudation into the interstitial space and alveoli.
Inappropriate ADH secretion is a contributing factor.
- Cardiogenic or fluid overload.
Bronchospasm:
Unopposed cholinergic bronchoconstrictor activity caused by loss of sympathetic innervation of the airway with unopposed parasympathetic activity.
Transection of the cervical spine interrupts the sympathetic nerve supply to the lungs, which originates from the upper 6 thoracic ganglia.
Parasympathetic innervation, arising from the vagal nuclei of the brainstem, remains intact.
It is concluded that resting airway tone is potentially increased in individuals with tetraplegia.
Hypersecretion of bronchial mucus:
Caused by the loss of sympathetic control and unopposed vagal activity.
Atelectasis:
It occurs secondary to
- Impaired expansion of lungs caused by weak respiratory muscles
- Abdominal content pushing cephalad
- Retained bronchial secretions
- Weak cough
- Reduction in the release of surfactant - Decreased inflation of the alveoli leads to a significant reduction in the release of surfactant.
Aspiration of gastric contents
Pneumonia
Pulmonary thrombo-embolism
There may be another class in between C3 and C 5 which leads to partial paralysis, usually needs assisted ventilation.
ReplyDeleteHowever, writing excellent .Huge information in a single page.
Thank you.
Hopefully next topic will be spinal shock
very informative.
ReplyDelete